
Symbien: article on Buildings
The Role of Mechanical Ventilation in Indoor Air Quality in Schools
Indoor air quality (IAQ) is a crucial factor for the well-being and mental and physical health of people in enclosed environments. This aspect has become increasingly important over the years, especially as building envelopes are designed to be more energy-efficient and airtight, as required, for example in Europe, by progressively stricter European EPBD Directives. Buildings with highly airtight envelopes, if not complemented by appropriate ventilation systems experience a deterioration
Go to the article
Introduction
Indoor air quality (IAQ) is a crucial factor for the well-being and mental and physical health of people in enclosed environments. This aspect has become increasingly important over the years, especially as building envelopes are designed to be more energy-efficient and airtight, as required, for example in Europe, by progressively stricter European EPBD Directives. Buildings with highly airtight envelopes, if not complemented by appropriate ventilation systems experience a deterioration in indoor air quality, leading to an increased risk of developing Sick Building Syndrome (SBS). A commonly used parameter for assessing indoor air quality is the concentration of CO2. This metric is essential in evaluating occupant well-being, especially in crowded spaces like daycares and schools, where monitoring becomes increasingly relevant. When carbon dioxide concentration reaches critical thresholds of 1000 ÷ 1500 ppm(v), it may become a health concern, leading to a decline in cognitive abilities and having a narcotic effect; for this reason, particular attention is given to settings such as schools and hospitals, which have been the focus of numerous analyses in the scientific literature.
Another aspect to consider when addressing IAQ is radon. Radon poses a signifi cant health risk, as it is estimated to cause more than 100,000 deaths worldwide annually and is the second leading cause of lung cancer deaths after cigarette smoking.
Conclusions
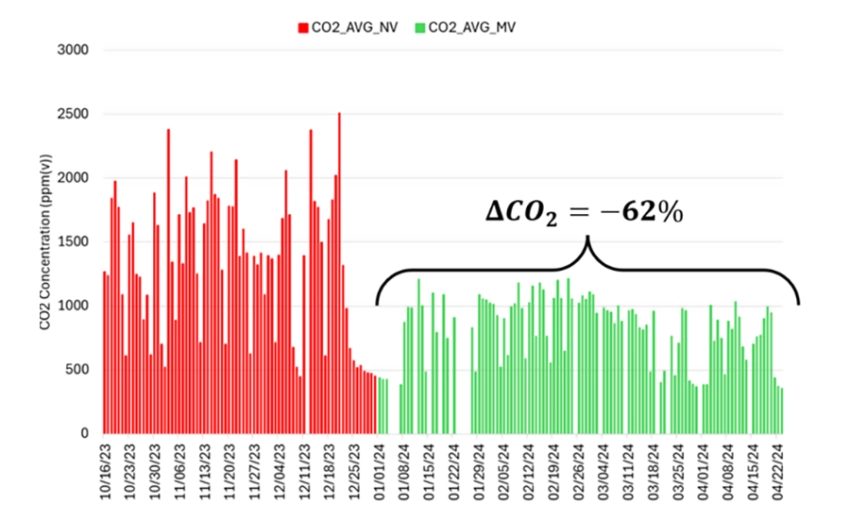
CO2 concentrations in the classroom dropped significantly with mechanical ventilation, with peak values reaching more than 4500 ppm(v) under natural ventilation and rarely exceeding 1500 ppm(v) with mechanical ventilation. The average concentration during occupancy decreased from around 2500 ppm(v) to levels close to 1000 ppm(v) and a reduction of 62% (Figure 10a, considering mean values during the occupation period), and the daily reduction reached −68% considering the maximum daily values.